Picture yourself receiving healthcare. Who is your physician? Do you see a man or a woman? That may depend on the medical specialty. If you are a woman seeing your gynecologist, do you see a man or woman? Likewise, if you are a man seeing your cardiologist, do you see a man or woman? Men and women are very different, and the medical workplace is no exception. For example, women display more empathy and use less medical slang compared to their male counterparts. These distinctions influence how patients choose their physicians. Patients may prefer a physician of the same gender since they are more comfortable expressing their emotions to build trust. In more empathy-based specialties, like psychiatry, the physician’s communication style is more important for better quality outcomes than their gender. Based on these differences, I evaluate the relationship between physician gender and quality measures in medical specialties.
I observe the presence of a female physician in three specialties: obstetrics and gynecology (OBGYN), family medicine, and cardiology. Why these three? In my data, I cannot access patient demographics. Since OBGYN focuses on women’s reproductive health, most patients are female. Cardiology is a male-dominated specialty since cardiovascular issues are undetected in women. Lastly, family medicine has a mix of male and female patients. In these specialties, I study the presence of female physicians to examine the gender mix and match between physician and patient as a result of the rising number of women in the healthcare workforce.
Figure 1 demonstrates the average percentage of female physicians in each practice compared to total practices before implementing quality measures. The patients in these practices are enrolled in Traditional Medicare insurance, which primarily covers people at least 65 years old. These practices do not reflect all people who need to see these physicians. When viewing Figure 1, note that there are 19,199 total practices. Of those total practices, 1,655 are family medicine practices, 462 are cardiology practices, and only 156 are OBGYN practices.

Cardiology has the lowest average volume of female physicians while OBGYN has the highest average percentage of female physicians, despite few reported practices. After analyzing the average female physicians, I separate the data based on the number of female physicians in the practice. For each specialty, I plot the average practice quality score. This allows me to directly examine how female physicians impact practice quality scores.
Different types of quality scores impact the final quality score. The final quality score determines the bonus or penalty providers receive based on the outcomes of the care provided. One aspect of the final score is the Quality Category Performance Score, which makes up 55% of the final score (in 2021). This measure evaluates how many activities a practice has implemented that teach patients components of preventive care for different illnesses. For example, do patients receive cognitive assessments? Are they educated about tobacco usage? Figure 2 demonstrates how a practice’s Quality Performance Category Score changes when increasing the volume of female physicians.
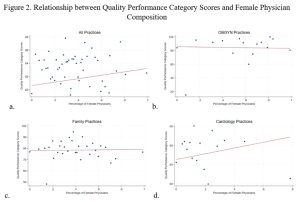
Through a regression analysis, all practices and, surprisingly, cardiology practices have statistically significant Quality Performance Category Scores once I control for physicians’ years of experience and state. “State” means I compare practices with different amounts of female physicians in the same state. The results show the complete opposite of what I hypothesized! In OBGYN practices, there seems to be a high, flat line. This is known as a “ceiling effect.” Gender did not impact outcomes, but these practices are so high-achieving that there is not much room for improvement. Contrarily, cardiology practices have a huge increase in quality outcomes when there are more female physicians!
Despite my original theory of gender match, gender mix actually creates better quality outcomes. It turns out the presence of a female physician is more important in a male-dominated specialty. Female physicians may help their male counterparts when engaging with patients, or male patients may respond better to female physicians. The high outcomes associated with gender mix show the need for physician diversity. Further research should assess how medical school students specialize, practice recruiting policies, how gender impacts quality in other specialties, and whether diverse races and ethnicities improve practice quality measures. Physician diversity is crucial to better healthcare quality.
Sophia Hottois is a junior honors student studying at the O’Neill School of Public and Environmental Affairs at Indiana University. She majors in Law and Public Policy with minors in Healthcare Management and Policy and Sports Marketing and Management. Sophia is a peer educator for the O’Neill Career Hub, a Statistics Tutor, and serves on the IU Student Government Supreme Court with the Office of Student Conduct.
Leave a Reply