
The United States is notorious for its extravagant spending on healthcare and the climbing costs of prescription drugs. In what seems to be a time of unjustifiable pharmaceutical price spikes, what is keeping pharmaceutical companies accountable?
The pharmaceutical industry is one of the most profitable sectors in the U.S., partly due to the minimal regulations imposed on it. Indeed, it is difficult to forget the actions of former Turing Pharmaceuticals CEO, Martin Shkreli, who suddenly raised the price of Daraprim from $13.50 to $750 per tablet when its generic form was not yet available in the U.S.
Pharmaceutical companies often justify these price spikes by stating their need to balance pricing with innovation—they need to be able to pay for future research and to cover costs of unsuccessful projects. There unfortunately is little information on how they do so.
This lack of transparency not only exists in price setting, but also in product marketing. Marketing is essential for fueling profits and compensating for the costs of innovation. Unsurprisingly, there has been a lack of accountability for pharmaceutical companies’ roles in direct-to-physician marketing—their primary method of sales promotion.
Direct-to-physician marketing is the promotion of pharmaceutical products to physicians. Most of these promotions are conducted by pharmaceutical sales representatives, who can give payments to physicians in the form of buying lunch, giving gifts, or giving out free drug samples in the time they have to discuss the product of interest.
Many are concerned about how these interactions influence prescribing habits. Did my physician (either consciously or subconsciously) choose to prescribe this drug to me because they truly think it is in my best interest, or did that charismatic pharmaceutical rep influence their choice? Without records of these financial exchanges, it is difficult to tell.
There were no national records, and therefore no accountability for these exchanges until 2010, when the Affordable Care Act introduced the Physician Payments Sunshine Act (PPSA).
The PPSA mandates that pharmaceutical manufacturers report any payments made to physicians valued over $10 or which sum to over $100 in a year. Information is then managed by the Centers for Medicare and Medicaid Services (CMS), who publishes the data online for public access.
I used these published financial records for 2014, 2015, and 2016, to evaluate possible pharmaceutical marketing strategies for antidepressants and anti-anxiety medications—one of the top most utilized prescriptions. I assessed whether pharmaceutical companies market these drugs based on a strategy of potential patients. That is, whether they market more to physicians working in communities that are more likely to contain patients who have depression and anxiety disorders, and are therefore more likely to utilize these medications.
I characterized these communities of potential patients using demographic and health factors. I then explored relationships between these factors and the amount of money physicians were paid for the marketing of antidepressants and anti-anxiety medications.
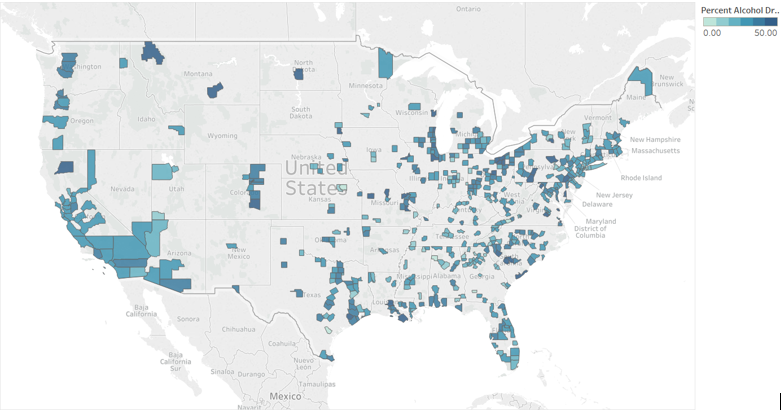
The demographic factors I evaluated were gender, elderly population, non-White Hispanic population, rural population, median household income, and those with some college education. The health factors of interest were physical inactivity, adult obesity, heavy drinking, and violence in the counties in which recipient physicians work.
Overall, the uneven distribution of payments to physicians by pharmaceutical companies demonstrated the existence of a specific marketing strategy. I found, however, that pharmaceutical marketing of antidepressants and anti-anxiety medications directly to physicians does not seem to be guided by the people these physicians are more likely to treat.
Independent analyses between the payment amounts received by physicians and the demographic or health characteristics of the people living near them revealed some relationships, but these were very minimal. Even when looking at all of these demographic and health factors together, rather than separately, there were still weak associations with the amount of money physicians were paid.
In terms of the locations of physician marketing, pharmaceutical companies marketed antidepressants and anti-anxiety medications to more rural areas, compared to the locations in which they marketed all types of medications. This might be connected to the potential for market growth.
The results imply that pharmaceutical companies do not market antidepressants and anti-anxiety drugs based on the potential pool of patients. That is, they do not mainly target physicians who are more likely to treat people with depression and anxiety.
This raises some questions then, as to what the actual marketing strategy is. Perhaps the uneven distribution of payments is dictated by how receptive physicians are to these interactions. Maybe companies market to physicians closer to company headquarters. Or perhaps they target areas with the greatest market growth potential.
Whatever the case, it is important that we use the newly available transparent financial records to continue to examine pharmaceutical-physician relationships. If we can understand pharmaceutical marketing strategies, then we may become aware of which people are most vulnerable to biased patient care.
After all, there is an inherent trust between a physician and a patient, but with minimal regulations, pharmaceutical companies threaten that trust while in pursuit of a profit. Research on these financial records, however, would help restore that trust by holding pharmaceutical companies accountable.
Leave a Reply