I am working on a proposal that may be of interest to NSF RAPID. My background in architecture, medical geography, location optimization and network science may help identify key scientific insights and spatial inefficiencies in hospital infections.
“
Hospital Infection Model — A Network Approach
If infections are due to exposure and exposure is a function of distance then infections can be reduced by optimizing travel behavior of infection agents (e.g. doctors, nurses, patients, germs) inside a hospital. We use the Sidney & Lois Eskenazi Hospital at Indiana University Purdue University Indianapolis to demonstrate an ~180 percent increase in ‘time to washing’ efficiency by using best optimal locations for hand washing. We simulated all probable pathways within the hospital architecture (all rooms, hallways, restrooms etc.) using Simulation Science (Polyak averaging), Computer Aided Design (CAD) and Geographic Information Science (GISc) to determine a globally optimal set of locations of disinfection stations (wash place, restrooms, detox stations etc.). We minimize distance to disinfection stations using Network Science, human behavior, Operations Research (p-medians), CAD & GISc. Preliminary results show large variations in distance to infection when sub-optimal locations for disinfection are used. Combining Network Science with Operations Research optimization approach we find best locations for disinfection. Presently, we apply completely chaotic movement behavior (completely deterministic billion plus routes) and robust stochastic optimization techniques to establish empirical proof and theoretical insights. Finally, we would like to show the ’emergent’ or tipping point behavior of COVID19 infections. This would entail obtaining a compendium of hospital floor plans (across all USA) to support the collection of critical ephemeral data and conduct research on an accelerated basis to fight COVID19. Researching confined geometrical and topological spaces will help us understand infection mechanics and would contribute directly to geographic and spatial theory, spatial science, location science and infection epidemiology. In addition, we will investigate the ’emergent’ properties (related to the Reproductive Number R0) in this confined spatial context. We would like to investigate the especially important ‘backward bifurcation and hysteresis’ principle of spatial models as it pertains to p-median optimization that contributes to infection control.
Sidney & Lois Eskenazi Hospital Floor Plan Architecture
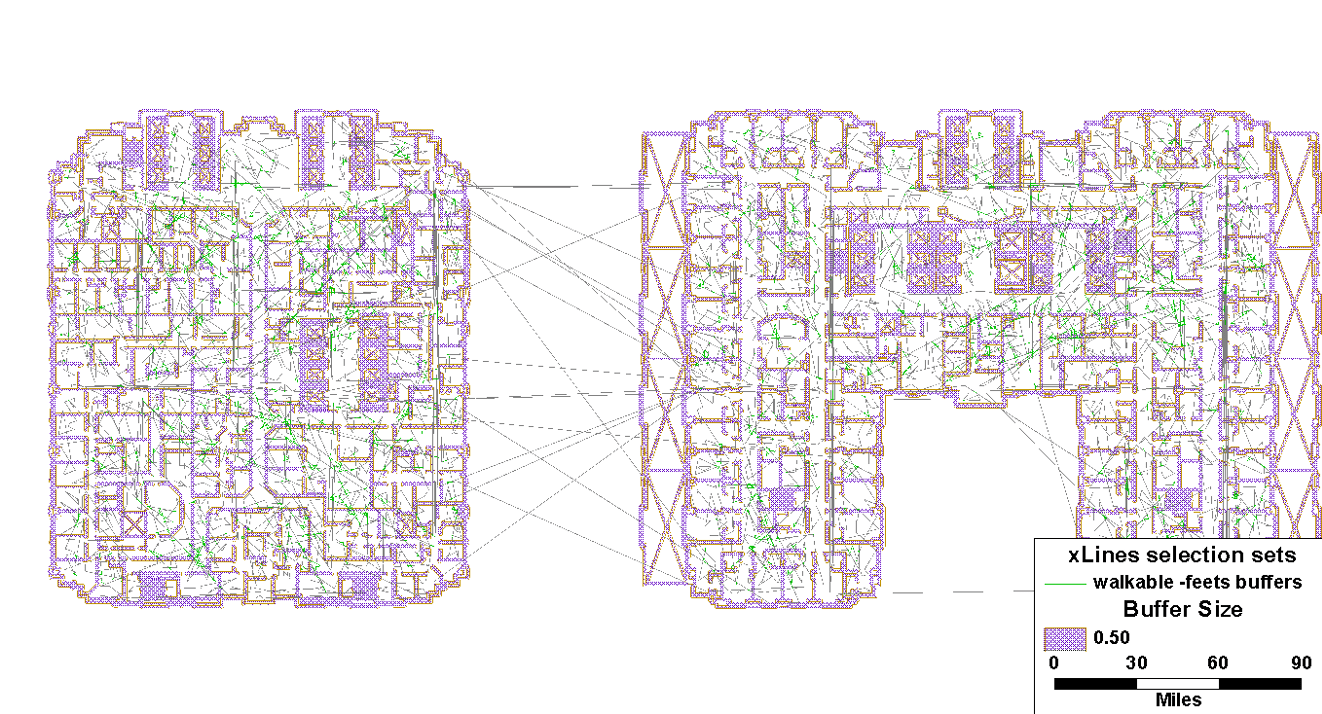

Simulation details of all possible trips inside a section of Hospital floor

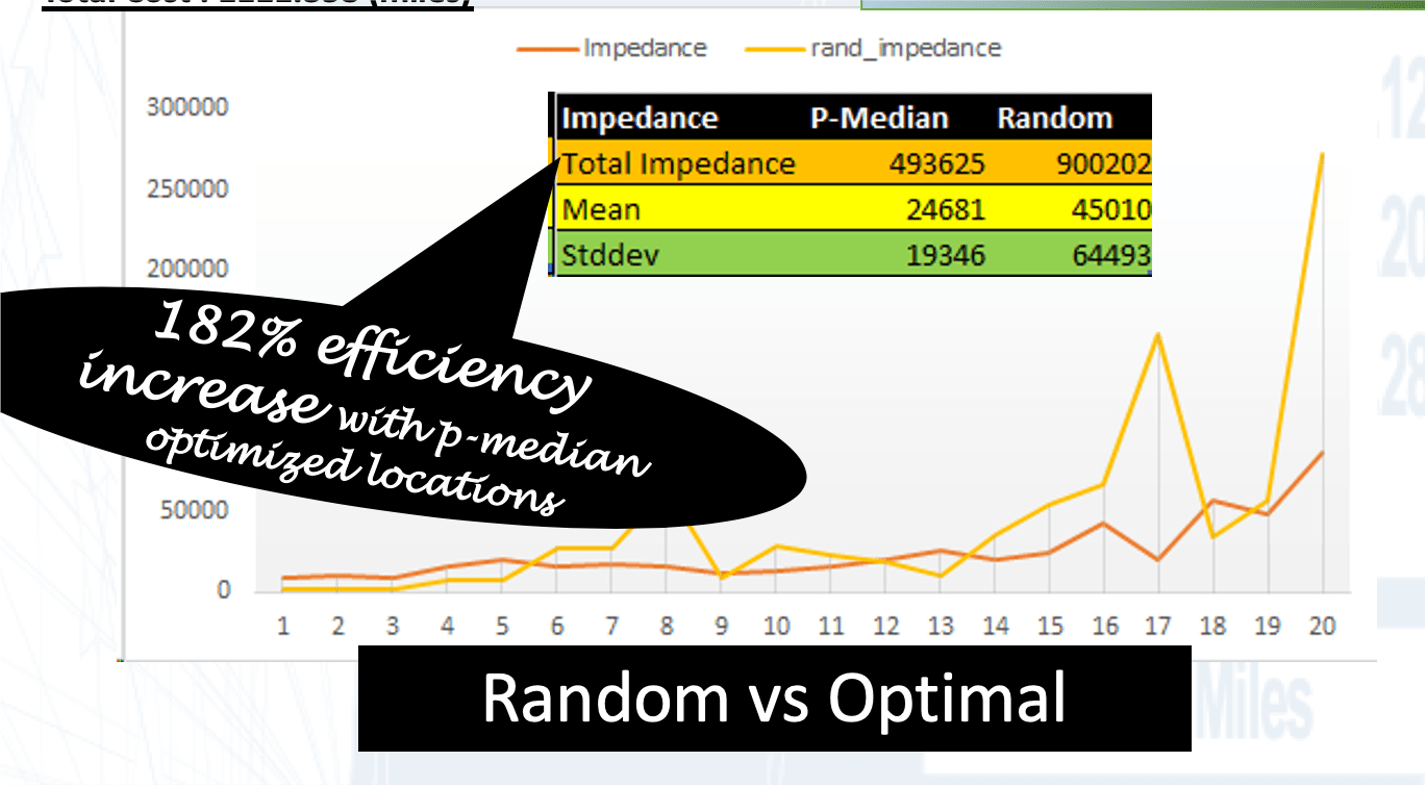
OPTIMALLY LOCATED STATIONS
- There is a 182 percent increase in efficiency (against legacy/random/unoptimized detox stations)
- i.e. a significant reduction between wash times
- If applied, there can be a significant reduction in Hospital Acquired infections related deaths
Subsequently, we would like to answer questions from real hospital data that we will collect, as follows:
(Based on hospital floor architecture, we have agents flowing through the network with some latent risk (asymptomatic) and some known risk (nodes w/ patients) and then you have nodes that reduce risk of agents flowing through (washing station). So then the network science questions are …)
- How do you rewire the network (architectural design) to reduce the spread of Covid19?
- How do you optimally place reduction nodes (washing stations) to reduce spread of Covid19?
- Where do you place known risk in the network (patients with Covid19) to minimize risk?
- How do you change behavior or the agents to reduce risk?
In addition, this optimization approach can be adopted to any floor plans like fire stations, office buildings, public places etc. with appropriate parameterization of infection propensities in the network nodes and weighted link nodes. We can join the micro-spatial CAD environment with the meso- & macro- spatial GISc environments to create seamless integration for a comprehensive infection control system for health inside and outside the hospital.”
[White Paper] Hospital Architecture and Preventing Infections: A Network Approach
[The NSF rapid can be a good fit for my NetSci 2018 Paris conference poster Hospital Architecture and Infection Modeling: A Network Approach see https://iu.box.com/s/4c38d79abqhyg9eeucxrc66gdrzhowrh]
- Abstract: If infections are due to exposure and exposure is a function of distance then infections can be reduced (preventative therapy) by optimizing travel behavior of infection agents (e.g. doctors, nurses, patients) inside the hospital. We simulate all probable pathways within the hospital architecture to determine a globally optimal set of locations of disinfection stations (wash place, restrooms, detox stations etc.) that minimizes infections using network/graph theory and GISc. Results show large variations in distance to infection when sub-optimal locations for disinfection are located. Using a graph theoretic integer programming optimization method we find optimal sets locations for disinfection. Presently, we apply completely chaotic movement behavior (completely deterministic) and use robust stochastic optimization techniques to establish further empirical proof.
- Keywords: network science, infection, agent based simulation, operations research, GISc, applied graph theory, hospital architecture.
Covid19 is a specific ‘leaf’ from the SARS-coV-2 ‘branch’ of the Coronavirus ‘tree’.
Nosocomial infections, like MRSA and possibly Covid19 (we don’t know the re-infection rates), are a result of treatment in a hospital, but secondary to the patient’s original condition.
- Before the Covid19 pandemic, the US CDC estimates that the total direct costs of such infections are above $17bn.
- Restating Kho (2008): virus innovate and cooperate and evolve and adapt to resist drugs and can transfer genetic traits between strains …
- For the first time, we apply network science, operations research, stochastic simulations of human behavior and Geographic Information Science to clearly demonstrate flawed hospital processes, including inappropriate sanitizer placements and poor hand washing by providers.
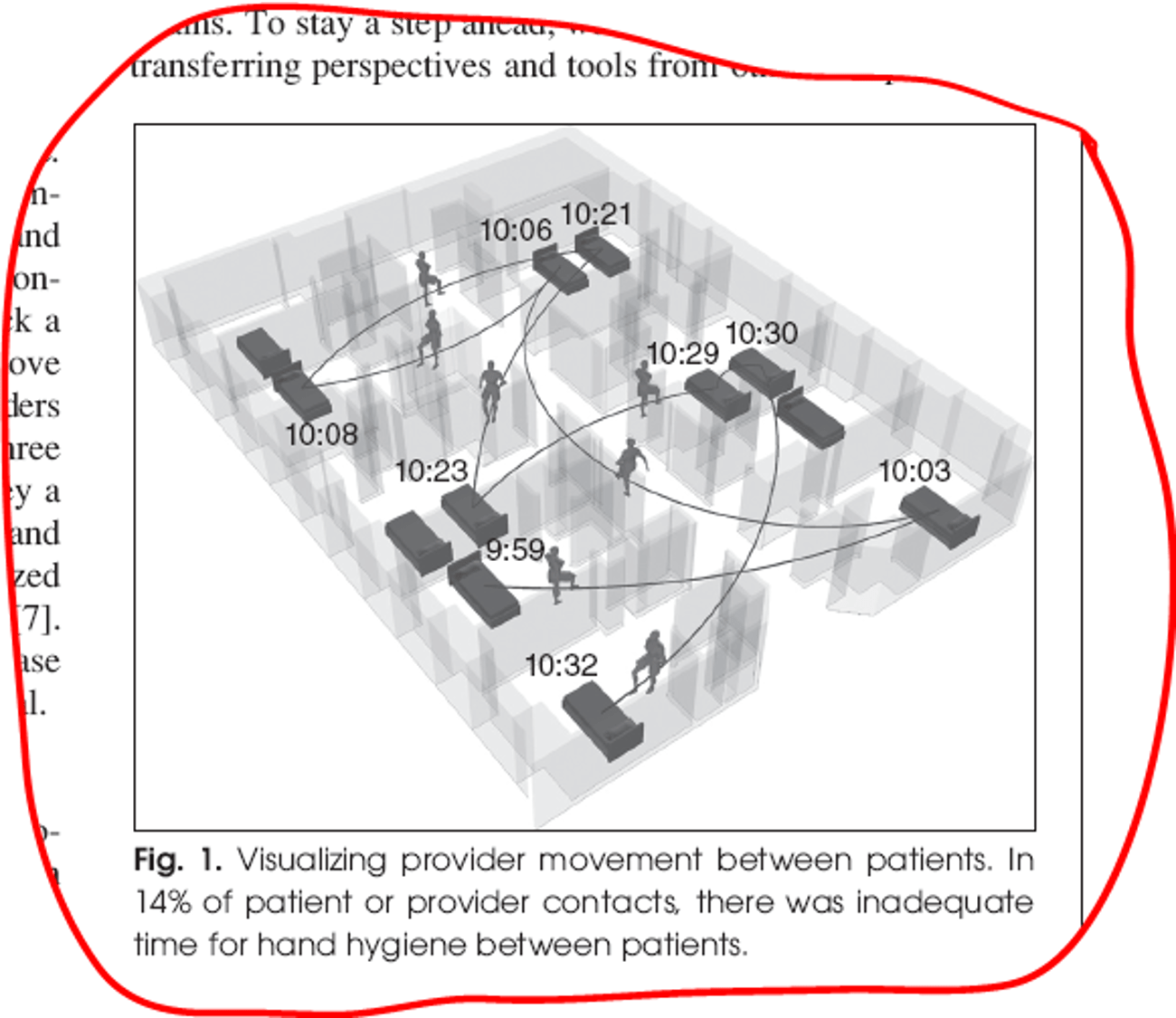
- Collecting bedside vital signs using the latest streamlined and automated processes is potentially increasing interpatient spread of infections.
- It is more important now than ever to provide access to sanitizers/restrooms/detox-units across hospital architecture in an optimal fashion.
- Using networks science, optimal sanitation units can potentially reduce MRSA infections. However, optimal locations can only be empirically derived using very large simulations and optimization algorithms as shown below.
Background
Methicillin-resistant Staphylococcus aureus (MRSA) is a bacterium responsible for difficult-to-treat infections in humans. It may also be referred to as multidrug-resistant Staphylococcus aureus or oxacillin-resistant Staphylococcus aureus (ORSA). MRSA is by definition a strain of Staphylococcus aureus that is resistant to a large group of antibiotics called the beta-lactams, which include the penicillins and the cephalosporins. MRSA/Methicillin Resistant Staphylococcus aureus was discovered in 1961 in the United Kingdom. It made its first major appearance in the United States in 1981 among intravenous drug users. MRSA is often referred to in the press as a “superbug“.

- Nosocomial infections are infections which are a result of treatment in a hospital or a healthcare service unit, but secondary to the patient’s original condition. Infections are considered nosocomial if they first appear 48 hours or more after hospital admission or within 30 days after discharge.Nosocomial comes from the Greek word nosokomeion (νοσοκομείον) meaning hospital (nosos = disease, komeo = to take care of). This type of infection is also known as a hospital-acquired infection (or more generically healthcare-associated infection).
- The Centers for Disease Control and Prevention (CDC) estimates that each year in the United States there are about 1.7 million nosocomial infections in hospitals and 99,000 associated deaths. The estimated incidence is 4.5 nosocomial infections per 100 admissions, with direct costs (at 2004 prices) ranging from $10,500 (£5300, €8000 at 2006 rates) per case (for bloodstream, urinary tract, or respiratory infections in immunocompetent patients) to $111,000 (£57,000, €85,000) per case for antibiotic resistant infections in the bloodstream in patients with transplants. With these numbers, conservative estimates of the total direct costs of nosocomial infections are above $17bn. The reduction of such infections forms an important component of efforts to improve healthcare safety (BMJ 2007).
 IEEE ENGINEERING IN MEDICINE AND BIOLOGY MAGAZINE 0739-5175/08/ ©2008IEEE NOVEMBER/DECEMBER 2008
IEEE ENGINEERING IN MEDICINE AND BIOLOGY MAGAZINE 0739-5175/08/ ©2008IEEE NOVEMBER/DECEMBER 2008- Not only that, Kho (2008) states: “Bacteria innovate and cooperate. They evolve and adapt to resist antibiotics and can transfer genetic traits between strains.”

Similarly, Covid19 is highly infectious and require similar sanitation.
Hospital Floor Plan Architecture
Simulation details of all possible trips inside a section of Hospital floor
OPTIMALLY LOCATED STATIONS
- There is a 182 percent increase in efficiency (against legacy/random/unoptimized detox stations)
- i.e. a significant reduction between wash times
- If applied, there can be a significant reduction in Hospital Acquired infections related deaths
APPENDIX
First, [A] we clarify with an Example. Second, [B] we Formalize and Compute the optimal solution.
[A] Example: Suppose there were five detox stations (hand-sanitizing stations, bathrooms etc.) in a hospital floor. Are they optimally location to reduce infections since distance to cleaning facility increases infections proportionately. We want to ‘optimally’ locate these facilities by minimizing the cost of walking to those stations for all travelers on all trips. Costs can be represented in terms of distance or travel times, representing trip impedance, and we can define five optimal “p-median” locations which simultaneously minimizes trip impedance for all locations assuming that every person on the hospital floor wishes to go to their nearest location – the “median” location – minimizing, in principle, the total cost of walking for all points of the floor. Now suppose that there are ‘n’ people walking from some location to these five outlets. The total distance traveled by each person to their nearest station can be measured using shortest paths to the nearest of the five median-based locations.
Not all trips are close to these stations. Trips away from these stations will face more distance and hence they are less accessible.
[B] Formalize and Compute optimal solution: Strategically placing five outlets in order to minimize the total distance traveled by all ‘n’ individuals is a challenging task. Randomly selected the five stations will not be optimal. However, methodically choosing all sets of five locations out of a typical floor with 100s of thousands of potential sites (of stations) provides a combinatorial problem that requires more than polynomial computation time O(Nk). This location problem is common in determining geographic locations of outlets and other businesses or services that wish to optimize locations relative travel patterns in urban settings and can be solved using a group of mathematical models called the p-median problem and is typically formulated as an Integer Program (IP) (ReVelle and Eiselt 2005)[1].
The least cost trip can be identified as that route which minimizes distances to the 5-locations. But we can also define a second least cost route, a third least cost route, and so on (i.e., called k-routes, where k=1 means the least cost one; e.g when we use Google routes they provide k=3 or 3 best routes ranked). Therefore, for any ‘p’-median location of outlets, ‘n’ people can take k-routes. In the mathematical optimization context, this translates into a parsimonious representation by using graph theory where: p-median (nodes), n people (nodes) and ‘k’ routes (links) form a network that can mathematically be investigated for optimal location of p-medians when k=1 (the shortest route chosen). Direct estimation of all possible k-routes would be an ideal way to simulate human behavior since people may not take or know the optimal route. In addition, solving this problem would take exponentially more computational time as number of people (n) increase (an NP-hard problem, (Reese, n.d.); (Schrijver 1986)). We can, however, simulate a sample of k-routes using computational methods and convert a well-defined deterministic but computationally hard problem into a probabilistic but computationally easy problem.
REFERENCES
Albert, Réka, Hawoong Jeong, and Albert-László Barabási. 2000. “Error and Attack Tolerance of Complex Networks.” Nature 406 (6794): 378–82. https://doi.org/10.1038/35019019.
Hakimi, S. L. 1965. “Optimum Distribution of Switching Centers in a Communication Network and Some Related Graph Theoretic Problems.” Operations Research 13 (3): 462–75.
ReVelle, C. S., and H. A. Eiselt. 2005. “Location Analysis: A Synthesis and Survey.” European Journal of Operational Research 165 (1): 1–19. https://doi.org/10.1016/j.ejor.2003.11.032.
Schrijver, Alexander. 1986. Theory of Linear and Integer Programming. USA: John Wiley & Sons, Inc.
Winston, Wayne, and Jeffrey Goldberg. 2004. Operations Research: Applications and Algorithms.

Leave a Reply